Understanding the True Source of Pain
You aim the fire extinguisher at the fire, not the alarm.
I use this metaphor often because where patients feel pain is not always where the pain originates. Excluding pathologies, many types of pain act like alarm, they alert you to a problem, but they don’t necessarily reveal the source. In most cases I see, the pain isn’t generated where it’s felt. Instead, it often results from faulty mechanics elsewhere in the body, creating abnormal stress in the painful area.
Pain is complex, yes, but it’s also real. And for lasting relief, we must uncover and treat its true cause.
Here are some examples where pain (the alarm) originates from a different location (the fire):
Trigger Point:
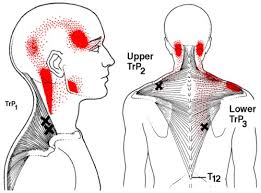
Trigger points are discrete, hyperirritable nodules located within taut bands of skeletal muscle. These can cause both local and referred pain. They often develop from acute trauma or repetitive strain, such as poor posture.
A classic example is a trigger point in the trapezius muscle that causes pain mimicking a headache. Applying pressure to these points often reproduces the patient’s pain. Fortunately, referred pain patterns from trigger points are well documented and predictable. Various soft tissue techniques can help release and deactivate these trigger points.
Sclerotogenous Pain:
This type of pain arises from deep structures and follows embryologic development patterns. It’s caused by irritation or compression of the sclerotome, which relates to the spinal region where sensory nerves exit.
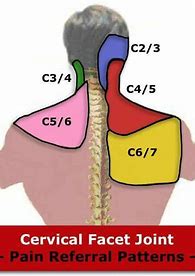
For example, irritation of the C6–C7 nerves in the neck can cause pain around the shoulder blade. Patients often describe this as mid-back pain, but the true source is the cervical spine. Treating the back may offer temporary relief, but without addressing the root in the neck, lasting improvement won’t happen.
Dermatomal Pain:
Dermatomal pain follows specific skin pathways, known as dermatomes, corresponding to spinal nerve roots. There are 24 pairs of spinal nerves, and irritation to any of them can cause predictable patterns of pain or sensory loss.
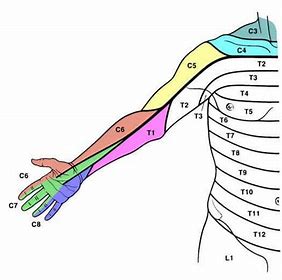
During a physical exam, tools like a pinwheel assess sensory integrity. For instance, decreased sensation in the left pinky may indicate an issue along the C8 nerve pathway. To relieve this type of pain, it’s critical to identify and treat the point of nerve irritation which can be anywhere along its path.
Compensatory Pain:
This is one of the most common forms of pain I encounter with joint injuries. Here, pain is experienced in a different part of the body than the actual source of the problem.
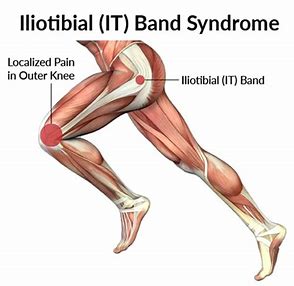
A common example is Iliotibial (IT) Band Syndrome, often presenting as lateral (outside) knee pain. The IT band is a long tendon along the outside of the thigh. It’s controlled by the Tensor Fascia Lata (TFL), a hip muscle responsible for stabilizing the pelvis and abducting the leg.
While the pain is felt at the knee (where the IT band inserts), the issue usually stems from dysfunction in the TFL or elsewhere along the kinetic chain. This condition is so prevalent in runners that it’s often called “runner’s knee.”
A Real-Life Case Study
One of my patients, a golfer, not a runner, came in with persistent lateral knee pain. Home remedies like ice, rest, and stretching weren’t helping. After ruling out meniscal or ligament damage, I diagnosed classic IT Band Syndrome.
We started treatment on the IT band, but relief was minimal. Next, I explored other possible contributing factors: the sciatic nerve, gluteal muscles, and sacroiliac (SI) joint. Again, some improvement, but still not enough.
Then I assessed the antagonist muscles to the TFL/IT band, the adductors, located on the inner thigh. There are four of them. I treated each one sequentially using Active Release Techniques® (ART®), retesting after each. When I finally worked on the smallest of the group, the pectineus, the patient’s knee pain vanished doing our provocative test. He couldn’t believe it.
Over the next few sessions, we focused on the pectineus and taught him specific stretches. That was the key. In 40 years of chiropractic practice, successfully treating hundreds of IT Band cases, this was the first one where the root cause was the pectineus muscle. I’ll never overlook it again.
Final Takeaway: Treat the Cause, Not Just the Pain
Just like aiming a fire extinguisher at the fire, not the alarm, we must aim treatment at the source of pain, not just where it’s felt.
Pain is complicated. But masking symptoms with medication, avoiding activity, or just “living with it” isn’t the answer. Find a healthcare provider who understands the musculoskeletal system, someone who will investigate and treat the root cause, so you can get back to doing the things you love.
If you have questions about your pain or want more information, feel free to email me at:
drbradweiss@performancehealthcenter.com